






Metformin Side Effects: What Indian Patients Should Know
Introduction Metformin is probably the most prescribed diabetes medication in India today, and for good reason. It is effective, affordable, has decades of safety data behind it, and works through a...

Introduction
Metformin is probably the most prescribed diabetes medication in India today, and for good reason. It is effective, affordable, has decades of safety data behind it, and works through a mechanism that addresses one of the core problems in Type 2 diabetes insulin resistance. Walk into almost any general physician’s clinic or endocrinology practice in India and you will find Metformin on the prescription pad. It is used not just for Type 2 diabetes but also for prediabetes, PCOS, metabolic syndrome, and in some cases as part of weight management protocols for patients with insulin resistance.
Table Of Content
- Introduction
- What Metformin Does in Your Body — And Why Side Effects Happen
- Common Side Effects of Metformin
- Gastrointestinal Side Effects — The Ones Most Patients Experience
- The Metallic Taste — Underreported but Real
- Appetite Changes and Weight
- Long-Term Side Effects of Metformin
- Vitamin B12 Deficiency — The Most Important Long-Term Risk
- Does Metformin Affect the Kidneys?
- Lactic Acidosis — Rare but Worth Understanding
- Metformin and PCOS — Side Effects in a Different Context
- Extended-Release Metformin — A Better Option for Many Indian Patients
- Why Indian Patients Specifically Need to Pay Attention
- When to Contact a Doctor
- Summary: Metformin Side Effects at a Glance
- Conclusion
- Frequently Asked Questions
Yet despite how commonly it is prescribed, a significant number of Indian patients stop taking Metformin within the first few weeks not because it stops working, but because the side effects in the early stages feel intolerable. Diarrhea, nausea, stomach cramps, bloating these are real and common, and when a patient is not told upfront that these symptoms are expected, temporary, and manageable, stopping the medication feels like the only logical response.
That decision stopping Metformin because of early side effects without medical guidance is one of the most preventable reasons for poor diabetes and PCOS management in India. At drcuro, we write about medical conditions and treatments specifically so that patients are informed before they encounter problems, not after. This guide covers everything Indian patients need to know about Metformin side effects: what they are, why they happen, how they differ by dose and formulation, what the long-term risks actually look like, and how the specific dietary and lifestyle patterns common in India interact with those risks.
What Metformin Does in Your Body — And Why Side Effects Happen
Before getting into specific side effects, it helps to understand what Metformin is actually doing inside your body because the mechanism explains most of the side effects directly.
Metformin works through three primary actions. First, it suppresses glucose production in the liver, which is the main driver of elevated fasting blood sugar in Type 2 diabetes. Second, it improves insulin sensitivity in peripheral tissues meaning your muscles and fat cells become more responsive to the insulin your pancreas is already producing. Third, it slows glucose absorption in the intestines, reducing the spike in blood sugar that follows a meal.
That third mechanism slowing intestinal glucose absorption is directly responsible for most of the gastrointestinal side effects patients experience. Metformin accumulates at relatively high concentrations in the gut wall, where it alters how intestinal cells process glucose and affects the composition of gut bacteria. This disruption to normal intestinal function is what causes diarrhea, nausea, bloating, and cramping in many patients, particularly at the beginning of treatment or when the dose is increased.
Importantly, these GI effects tend to diminish over time as the gut adapts. Most patients who push through the first two to four weeks find that symptoms reduce significantly or disappear entirely. The problem is that many patients are not told this upfront so they stop the medication during exactly the window where symptoms are worst and improvement is closest.
Common Side Effects of Metformin
Gastrointestinal Side Effects — The Ones Most Patients Experience
The gastrointestinal side effects of Metformin are by far the most common category. Research estimates that anywhere from 20 to 30 percent of patients experience significant GI symptoms when starting Metformin, with some studies putting the figure higher depending on the starting dose.
Diarrhea is the single most frequently reported side effect. It can range from mildly loose stools to urgent, frequent bowel movements that significantly disrupt daily life. For Indian patients specifically, diarrhea caused by Metformin can be particularly disruptive because of the social and professional contexts in which it occurs long commutes, office environments without easy bathroom access, and social eating situations where sudden urgency is embarrassing. The diarrhea is typically worse in the first one to two weeks and improves substantially thereafter, though for a subset of patients it persists at a lower level throughout treatment.
Nausea is the second most common complaint. It usually occurs within an hour or two of taking the tablet and is more pronounced when Metformin is taken on an empty stomach. Many patients describe it as a low-grade but persistent sick feeling rather than acute vomiting, though in some cases nausea is severe enough to cause actual vomiting, particularly at higher doses.
Bloating, gas, and abdominal cramps round out the typical GI picture. These symptoms are caused by altered fermentation of carbohydrates in the large intestine Metformin changes how the gut microbiome processes certain sugars, leading to increased gas production. For Indian patients whose diets tend to be higher in complex carbohydrates rice, dal, roti, pulses this effect can be more pronounced than in patients eating lower-carbohydrate Western diets.
| GI Side Effect | How Common | Timing | Typical Duration |
| Diarrhea | Very common (20–30%) | Within days of starting | 2–4 weeks, often resolves |
| Nausea | Common (15–25%) | 1–2 hours post-dose | 1–3 weeks, often resolves |
| Bloating | Common | First 1–2 weeks | Usually temporary |
| Abdominal cramps | Moderate (10–15%) | Variable | Usually temporary |
| Vomiting | Less common | Shortly after dose | Contact doctor if persistent |
| Loss of appetite | Common | First few weeks | Often persists modestly |
| Metallic taste | Less common | Variable | Often resolves |
Practical steps that genuinely reduce GI side effects:
- Always take Metformin with food not before, not after, but during a meal. This single step reduces GI symptoms more than almost anything else.
- Start at the lowest effective dose (usually 500mg once daily) and increase slowly over several weeks rather than jumping to the full prescribed dose immediately. Many Indian patients are started on 500mg twice daily right away if your doctor agrees, asking to start at 500mg once daily for the first week can significantly ease the transition.
- Avoid taking Metformin with a particularly heavy, oily, or spicy meal the combination of a high-fat meal and Metformin tends to worsen nausea and diarrhea.
- Stay well hydrated, especially important during Indian summers where dehydration can concentrate the medication’s GI effects.
- If symptoms are severe, speak to your doctor about switching to extended-release Metformin (discussed in detail later in this article) before deciding to stop treatment altogether.
The Metallic Taste — Underreported but Real
A side effect that patients rarely mention unprompted because it seems minor compared to diarrhea is a persistent metallic or bitter taste in the mouth. It affects a minority of Metformin users but can be genuinely unpleasant, particularly because it alters the taste of food. For Indian patients for whom food is culturally central and meals are social events, a medication that makes food taste wrong is worth acknowledging.
The metallic taste tends to be most prominent in the first few weeks and fades for most patients over time. Staying well hydrated, chewing sugar-free gum between meals, and rinsing with water after taking the tablet can help reduce the sensation. It is not dangerous and does not indicate anything wrong with how the medication is working.
Appetite Changes and Weight
Metformin commonly reduces appetite, particularly in the early weeks of treatment. This is partly a direct effect of nausea reducing the desire to eat, and partly a metabolic effect of improved insulin sensitivity reducing hunger signals. For overweight patients with Type 2 diabetes or PCOS a common presentation in India this appetite reduction is often welcomed and contributes to modest weight loss.
However, it is important to be clear about what Metformin does and does not do regarding weight. It is not a weight-loss medication. The average weight loss associated with Metformin is modest — typically 1 to 3 kilograms over several months — and highly variable between individuals. Some patients lose more, many lose nothing at all. Metformin should never be relied upon as a primary weight management strategy, and patients should not increase their dose in the hope of accelerating weight loss. At drcuro, we emphasize this point because misinformation about Metformin and weight loss is widespread in Indian health communities, including in WhatsApp groups and social media, where exaggerated claims about its slimming effects circulate regularly.
Long-Term Side Effects of Metformin
The short-term GI side effects get most of the attention, but the more clinically significant concern with long-term Metformin use is something patients rarely hear about: Vitamin B12 deficiency.
Vitamin B12 Deficiency — The Most Important Long-Term Risk
Metformin reduces the absorption of Vitamin B12 in the small intestine by interfering with a specific calcium-dependent absorption mechanism. This is a well-established, dose-dependent effect the longer you take Metformin and the higher your dose, the greater the reduction in B12 absorption over time. Studies suggest that between 10 and 30 percent of long-term Metformin users develop biochemical B12 deficiency, though many remain asymptomatic for years before the deficiency becomes clinically apparent.
This matters particularly for Indian patients for two reasons. First, India already has one of the highest rates of Vitamin B12 deficiency in the world, driven by the prevalence of vegetarian and vegan diets across large sections of the population. B12 is found almost exclusively in animal products — meat, fish, eggs, and dairy. A patient who is already borderline deficient in B12 before starting Metformin is at significantly higher risk of developing a clinically meaningful deficiency once the medication further impairs absorption. Second, B12 deficiency is frequently underdiagnosed in India because its symptoms fatigue, weakness, tingling in the hands and feet, memory problems, and mood changes are vague and commonly attributed to other causes including stress, anaemia, or simply overwork.
Symptoms of Vitamin B12 deficiency to watch for:
- Persistent fatigue and weakness that does not improve with rest
- Tingling, numbness, or a pins-and-needles sensation in the hands or feet
- Difficulty walking or problems with balance
- Memory problems, difficulty concentrating, or brain fog
- Mood changes including low mood or irritability
- A sore, inflamed tongue (glossitis)
- Pale or slightly yellowed skin
| Risk Factor for B12 Deficiency | Relevance to Indian Patients |
| Vegetarian or vegan diet | Very high relevance — large proportion of Indian population |
| Long-term Metformin use (>3 years) | Directly applicable |
| Higher Metformin dose (>1500mg/day) | Common in poorly controlled diabetes |
| Older age | Relevant — B12 absorption declines with age |
| Pre-existing low B12 levels | Common in India even without Metformin |
| Gastric issues affecting absorption | Relevant — H. pylori infection is common in India |
What should be done:
- Ask your doctor to check your Vitamin B12 level before starting Metformin and then annually if you are on long-term treatment
- If you are vegetarian or vegan, discuss B12 supplementation proactively do not wait until a deficiency develops
- B12 supplementation is safe, inexpensive, and highly effective at preventing deficiency oral supplements work for most patients, though injections may be needed for severe deficiency
- Do not self-diagnose and self-supplement without testing first B12 levels should guide the approach
Does Metformin Affect the Kidneys?
This is one of the most common concerns Indian patients raise, and it is frequently misunderstood in both directions some patients think Metformin damages kidneys, while others take it without any awareness of the kidney-related precautions that are genuinely important.
To be clear: Metformin does not damage healthy kidneys. It does not cause kidney disease. However, Metformin is eliminated from the body entirely through the kidneys, and in patients whose kidneys are already significantly impaired, the medication can accumulate to levels that increase the risk of a rare but serious complication called lactic acidosis.
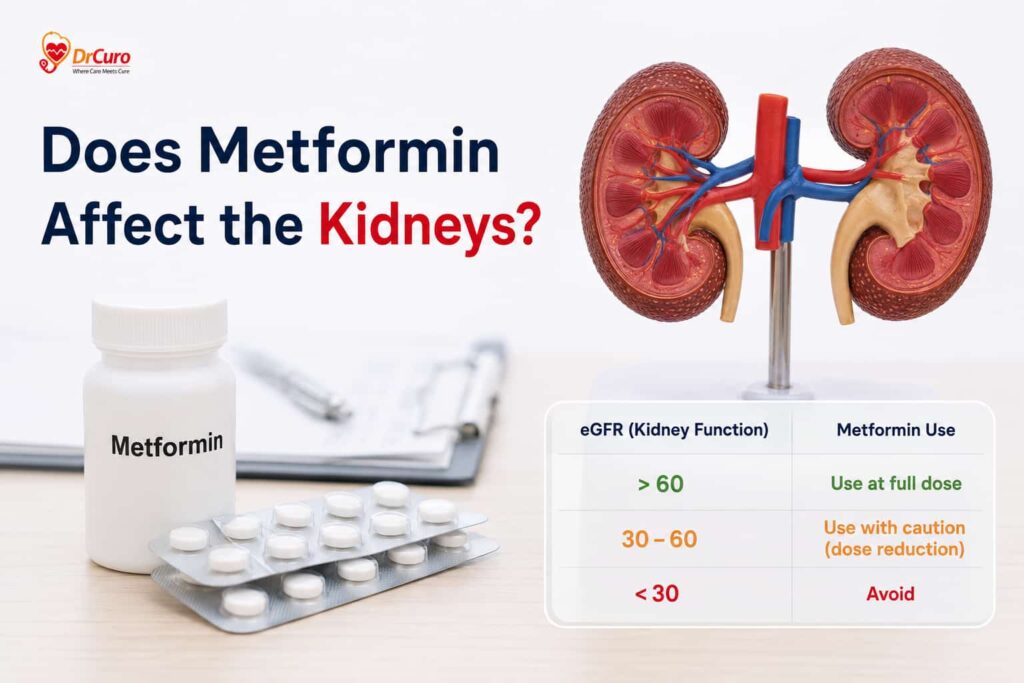
For this reason, Metformin doses are reduced or the medication is stopped entirely in patients with significant chronic kidney disease (CKD). Current guidelines suggest Metformin can be used safely at full doses when eGFR (a measure of kidney function) is above 60, should be used with caution and dose reduction when eGFR is 30–60, and should be avoided when eGFR is below 30.
In India, where chronic kidney disease secondary to diabetes and hypertension is extremely common and often underdiagnosed, this matters. Patients with diabetes who have never had their kidney function tested should ask for an eGFR test not because Metformin is causing kidney damage, but because existing kidney impairment changes how safely Metformin can be used.
Lactic Acidosis — Rare but Worth Understanding
Lactic acidosis is the complication that gets mentioned in every Metformin package insert and causes significant anxiety in patients who read it. It deserves honest context rather than either dismissal or alarm.
Lactic acidosis is a dangerous buildup of lactic acid in the blood. It is associated with Metformin but is genuinely extremely rare in patients who do not have the specific risk factors that make it more likely. The estimated incidence is approximately 3 to 10 cases per 100,000 patient-years meaning most patients on Metformin will never encounter it.
Risk factors that increase lactic acidosis risk:
| Risk Factor | Why It Matters |
| Severe kidney disease | Metformin accumulates; cannot be cleared |
| Significant liver disease | Liver cannot clear lactate effectively |
| Heavy alcohol consumption | Alcohol itself promotes lactic acid production |
| Severe dehydration | Reduces kidney clearance of Metformin |
| Severe infection or sepsis | Increases lactate production throughout body |
| Recent contrast dye procedure | Contrast can temporarily impair kidney function |
| Cardiac or respiratory failure | Reduces tissue oxygen delivery |
Warning symptoms of lactic acidosis — seek emergency care immediately if these occur:
- Extreme unexplained weakness or fatigue
- Rapid or labored breathing
- Severe muscle pain or cramping
- Stomach pain with nausea and vomiting
- Feeling cold or dizzy
- Irregular heartbeat
- Confusion or difficulty thinking clearly
The practical takeaway for Indian patients is straightforward: if you do not have significant kidney disease, liver disease, or heavy alcohol use, your risk of lactic acidosis on standard Metformin doses is extremely low. The risk becomes relevant when underlying health conditions that impair the body’s ability to clear Metformin or manage lactate are present and those conditions should already be on your doctor’s radar.
Metformin and PCOS — Side Effects in a Different Context
A significant proportion of Indian women taking Metformin are taking it not for diabetes but for PCOS. The side effect profile is the same, but the context is different in ways that matter.
Women with PCOS using Metformin are often younger, often not overweight (lean PCOS is common in Indian women), and are frequently using Metformin specifically to regulate menstrual cycles, reduce androgen levels, or improve ovulation for fertility purposes. The doses used in PCOS are typically lower than in diabetes management often 500mg to 1500mg daily which generally means milder GI side effects.
However, PCOS patients on Metformin face a specific concern that diabetes patients do not: many are of reproductive age and may become pregnant while on the medication. Metformin is generally considered safe in early pregnancy and is sometimes continued into the first trimester under specialist supervision, but this is a decision that should be made with a doctor not assumed to be fine because “it’s just Metformin.”
For Indian women with PCOS, the Vitamin B12 issue is particularly relevant if they are vegetarian, as discussed above. Additionally, the GI side effects of Metformin can be harder to tolerate in women who are also experiencing the nausea and bloating that PCOS itself sometimes causes, or in women who are trying to conceive and experiencing early pregnancy symptoms that are difficult to distinguish from medication side effects.
Extended-Release Metformin — A Better Option for Many Indian Patients
Standard Metformin (immediate-release) releases the medication quickly after swallowing, leading to high concentrations in the gut within a short window which is precisely why GI side effects are most intense with this formulation.
Extended-release Metformin (sold in India under various brand names and often written as Metformin XR or SR on prescriptions) releases the medication slowly over 8 to 10 hours. This produces lower peak concentrations in the gut at any given time, which significantly reduces the severity of diarrhea, nausea, and bloating for many patients.
| Feature | Standard Metformin | Extended-Release Metformin |
| Release mechanism | Immediate | Slow, over 8–10 hours |
| GI side effect severity | Higher | Lower |
| Dosing frequency | Usually twice or three times daily | Usually once daily (with evening meal) |
| Blood sugar control | Equivalent | Equivalent |
| Cost | Lower | Slightly higher |
| Availability in India | Widely available | Available, though fewer brands |
| Best for | Patients who tolerate it well | Patients with significant GI side effects |
Extended-release Metformin is not a different medication it is the same drug delivered differently. Blood sugar control is equivalent between formulations. The only meaningful differences are tolerability and cost. If you are struggling with GI side effects on standard Metformin, it is absolutely worth asking your doctor whether switching to the extended-release formulation is appropriate for you, rather than stopping Metformin altogether.
Why Indian Patients Specifically Need to Pay Attention
The standard Metformin side effect information written for Western patients is not wrong for Indian patients, but it misses several India-specific dimensions that genuinely matter.
Dietary interactions are more pronounced. The Indian diet is typically higher in refined carbohydrates white rice, maida-based bread, potatoes than the diets used in the Western clinical trials that generated most Metformin safety data. High carbohydrate intake alongside Metformin can worsen bloating and gas because there is more substrate available for the altered fermentation that Metformin causes in the gut. This does not mean Indian patients cannot take Metformin millions do so successfully every day but it does mean that dietary adjustments during the early weeks of treatment may be particularly helpful.
Irregular meal timing is a real problem. Many Indian patients skip breakfast, eat a very late lunch, or have long gaps between meals for cultural, professional, or religious reasons. Taking Metformin without food significantly worsens GI side effects. During Navratri fasting, Ramadan, or other religious observances involving extended fasting, patients need specific guidance from their doctor about how to manage Metformin this is not addressed in any standard Western prescribing guidance.
Self-medication culture creates specific risks. India has a significant self-medication culture, and Metformin is available over the counter at many pharmacies without a prescription. Patients who start Metformin without medical guidance are less likely to receive instructions about taking it with food, starting at a low dose, or monitoring for B12 deficiency. They are also more likely to adjust or stop the medication without professional input when side effects occur.
The vegetarian B12 deficiency risk cannot be overstated. As discussed earlier, the combination of a vegetarian diet and long-term Metformin use creates a compounding B12 deficiency risk that is far more relevant to the Indian population than to the Western populations in which most Metformin research was conducted.
When to Contact a Doctor
Most Metformin side effects are manageable at home with the strategies outlined above. But certain symptoms require prompt medical attention rather than a wait-and-see approach.
Contact your doctor if:
- Diarrhea is severe, bloody, or persists beyond four weeks without improvement
- You are vomiting and cannot keep the medication down
- You experience significant unexplained weight loss
- You develop symptoms suggestive of B12 deficiency tingling, numbness, persistent fatigue
- You are scheduled for surgery or a procedure involving contrast dye Metformin usually needs to be paused temporarily
- You develop a serious infection, severe dehydration, or are hospitalized for any reason
- You become pregnant or are planning pregnancy
Seek emergency care immediately if:
- You experience sudden severe weakness, difficulty breathing, muscle pain, or confusion these are potential signs of lactic acidosis and require urgent assessment regardless of how unlikely it seems
Summary: Metformin Side Effects at a Glance
| Side Effect | Frequency | Severity | Manageable? | Resolves Over Time? |
| Diarrhea | Very common | Mild to moderate | Yes | Usually |
| Nausea | Common | Mild to moderate | Yes | Usually |
| Bloating and gas | Common | Mild | Yes | Usually |
| Abdominal cramps | Moderate | Mild | Yes | Usually |
| Metallic taste | Less common | Mild | Partially | Often |
| Loss of appetite | Common | Mild | Generally yes | Partially |
| Vitamin B12 deficiency | 10–30% long-term | Moderate to serious | Yes with monitoring | No — requires supplementation |
| Low blood sugar | Rare (alone) | Variable | Yes | N/A |
| Lactic acidosis | Very rare | Serious | Preventable with screening | N/A — requires emergency care |
Conclusion
Metformin is not a perfect medication no medication is. Its gastrointestinal side effects are real, they are common in the early weeks, and they are the main reason Indian patients stop taking it prematurely. But they are also temporary for the vast majority of patients, manageable with straightforward adjustments to timing and diet, and worth pushing through given how effective Metformin is at the underlying condition it treats.
The more serious long-term concern Vitamin B12 deficiency is genuinely underappreciated in India, where the risk is compounded by dietary patterns that already make B12 deficiency common in the general population. Annual B12 monitoring for anyone on long-term Metformin is not optional box-ticking; it is clinically important.
At drcuro, our goal is to give Indian patients the specific, honest information they need to make informed decisions about their health not generic content written for a different population and applied wholesale to India. Metformin works. Understanding its side effects, managing them properly, and monitoring for the ones that matter long-term is what allows it to keep working safely for years. If you are taking Metformin and experiencing side effects, the answer is almost never to stop without speaking to your doctor first. The answer is almost always to understand what is happening, why it is happening, and what can be done about it.
Frequently Asked Questions
1. What is the most common Metformin side effect in Indian patients? Diarrhea is the most frequently reported side effect, affecting roughly 20–30% of patients when they first start treatment. It is most common in the first two weeks and improves significantly for most patients after that.
2. Should Metformin be taken before or after food? Always with food ideally during a meal, not before or after. This is the single most effective way to reduce nausea and diarrhea. Taking it on an empty stomach significantly worsens GI symptoms.
3. Can vegetarian Indian patients take Metformin safely? Yes, but they need to be more vigilant about Vitamin B12 monitoring than non-vegetarians. Vegetarians already have lower dietary B12 intake, and Metformin further impairs B12 absorption. Annual B12 testing and proactive supplementation if levels are low is strongly advisable.
4. Does Metformin damage the kidneys? No. Metformin does not cause kidney damage. However, patients with existing significant kidney disease need dose adjustments or may need to use an alternative medication, because impaired kidneys cannot clear Metformin efficiently.
5. What is extended-release Metformin and is it better? Extended-release Metformin releases the drug slowly over 8–10 hours rather than all at once, which significantly reduces GI side effects for many patients. Blood sugar control is equivalent to standard Metformin. If you are struggling with diarrhea or nausea, ask your doctor about this option before stopping treatment.
6. Can I take Metformin during religious fasting? This needs to be discussed with your doctor before the fasting period begins. Taking Metformin without food worsens side effects, and prolonged fasting changes how the medication behaves in your body. Your doctor may recommend timing adjustments or temporary dose changes during fasting periods.






No Comment! Be the first one.