






PCOS Renamed to PMOS? The Real Science Behind the Controversial Change
If you have been living with PCOS Polycystic Ovary Syndrome you have probably already heard the word more times than you can count. You have heard it from your doctor, read it on health websites,...

If you have been living with PCOS Polycystic Ovary Syndrome you have probably already heard the word more times than you can count. You have heard it from your doctor, read it on health websites, and maybe even searched it at 2 AM when you could not understand why your periods were irregular, why your weight would not budge, or why your skin kept breaking out. PCOS has been a familiar term for decades. But now, something surprising is happening in the world of medicine researchers and doctors are beginning to talk about replacing PCOS with a new name: PMOS, which stands for PolyMetabolic Ovary Syndrome. This has naturally created a lot of confusion and a lot of questions.
Table Of Content
- What Is PCOS and Why Have So Many Women Been Diagnosed With It?
- Why Is the Name PCOS Considered Outdated by Many Experts?
- What Does PMOS Mean and What Is the Difference?
- PCOS vs PMOS — A Simple Comparison
- Is PCOS Officially Renamed to PMOS? The Honest Answer
- The Hidden Danger — Why Metabolic Problems Are Often Missed
- What Does This Mean for Fertility?
- What Can You Actually Do — Lifestyle Changes That Make a Real Difference
- Foods That Help vs Foods That May Worsen Symptoms
- Common Myths About PCOS That Need to Be Corrected
- The Emotional and Mental Health Side of PCOS
- When Should You See a Doctor?
- Frequently Asked Questions
- What Actually Matters for Your Health
At drcuro, we understand how confusing and stressful it can be when medical information keeps changing. So in this blog, we are going to break everything down for you in the simplest possible way no complicated medical words, no unnecessary jargon. We will explain what PCOS actually is, why doctors feel the name is becoming outdated, what PMOS means, and most importantly, what all of this means for you and your health.
What Is PCOS and Why Have So Many Women Been Diagnosed With It?
PCOS, or Polycystic Ovary Syndrome, is one of the most common hormonal disorders in women of reproductive age. Estimates suggest that between 8 and 13 percent of women worldwide may have PCOS, though many cases go undiagnosed because the symptoms are so varied and can look like many other conditions. The name itself comes from the appearance of the ovaries on an ultrasound they often show multiple small follicles that look like tiny cysts arranged around the outer edge of the ovary. But here is something important that many women are not told: these are not dangerous cysts. They are actually immature follicles tiny egg sacs that did not fully develop and release an egg the way they should have.
This is the very first problem with the name PCOS. The word “polycystic” sounds alarming. Many women panic when they hear it, imagining that their ovaries are full of dangerous, painful cysts that might need surgery or lead to cancer. In reality, the situation is usually far less dramatic than the name suggests. These follicles are a result of hormonal imbalance, not a dangerous cyst disease. And to make things even more confusing some women who are diagnosed with PCOS do not even show these follicles on their ultrasound at all, yet they still have all the other symptoms of the condition.
Common symptoms of PCOS include:
- Irregular or missing periods
- Delayed or absent ovulation
- Difficulty getting pregnant
- Unexplained weight gain, especially around the belly
- Acne that does not respond well to usual treatments
- Excess facial or body hair (a condition called hirsutism)
- Hair thinning or hair loss from the scalp
- Dark patches of skin around the neck, underarms, or groin
- Constant fatigue and low energy
- Mood swings, anxiety, and depression
- Strong sugar cravings
- High levels of male hormones like testosterone
Why Is the Name PCOS Considered Outdated by Many Experts?
The term PCOS has been in use since the 1930s. Back then, doctors understood it primarily as a condition related to the ovaries and reproductive system. But science does not stay still. Over the past few decades, research has revealed that PCOS is far more complex than anyone originally thought. It is not simply an ovary problem. It is a whole-body condition that deeply involves the metabolic system meaning how the body processes food, manages energy, controls blood sugar, and responds to insulin.
One of the most significant discoveries in modern PCOS research is the role of insulin resistance. Studies show that between 65 and 70 percent of women with PCOS have insulin resistance, regardless of their body weight. This means their bodies produce insulin normally, but the cells in the body do not respond to it properly. As a result, the pancreas has to produce even more insulin to compensate. This excess insulin then signals the ovaries to produce more male hormones like testosterone, which disrupts ovulation, worsens acne, causes hair changes, and contributes to weight gain. It is a cascade effect — one thing triggers another.
The problem, then, is that the name PCOS draws all the attention to the ovaries. It makes doctors and patients think of it as a reproductive problem. But by the time a woman notices her irregular periods, the real root cause insulin resistance and metabolic dysfunction may have been brewing silently for years. At drcuro, we often see women who come to us focused entirely on their fertility, but when we dig deeper, we find that their blood sugar control, cholesterol levels, and liver health also need attention. The name PCOS simply does not prepare women or their doctors to look at the full picture.
What Does PMOS Mean and What Is the Difference?
PMOS stands for PolyMetabolic Ovary Syndrome. The key word here is “metabolic.” This proposed new name acknowledges what modern research has made clear: that the metabolic system specifically how the body handles insulin, blood sugar, fat storage, and inflammation is at the very core of this condition. The ovaries are affected, yes. But they are often a consequence of metabolic dysfunction, not the starting point.
Think of it this way. Imagine a river that keeps overflowing its banks and flooding nearby homes. The old name PCOS would be like calling it “Flooded Homes Syndrome” focusing on the visible damage. The new proposed name PMOS is more like “Blocked River Syndrome” pointing to the actual cause upstream. By naming the root problem, you give doctors and patients a much better chance of addressing it correctly.
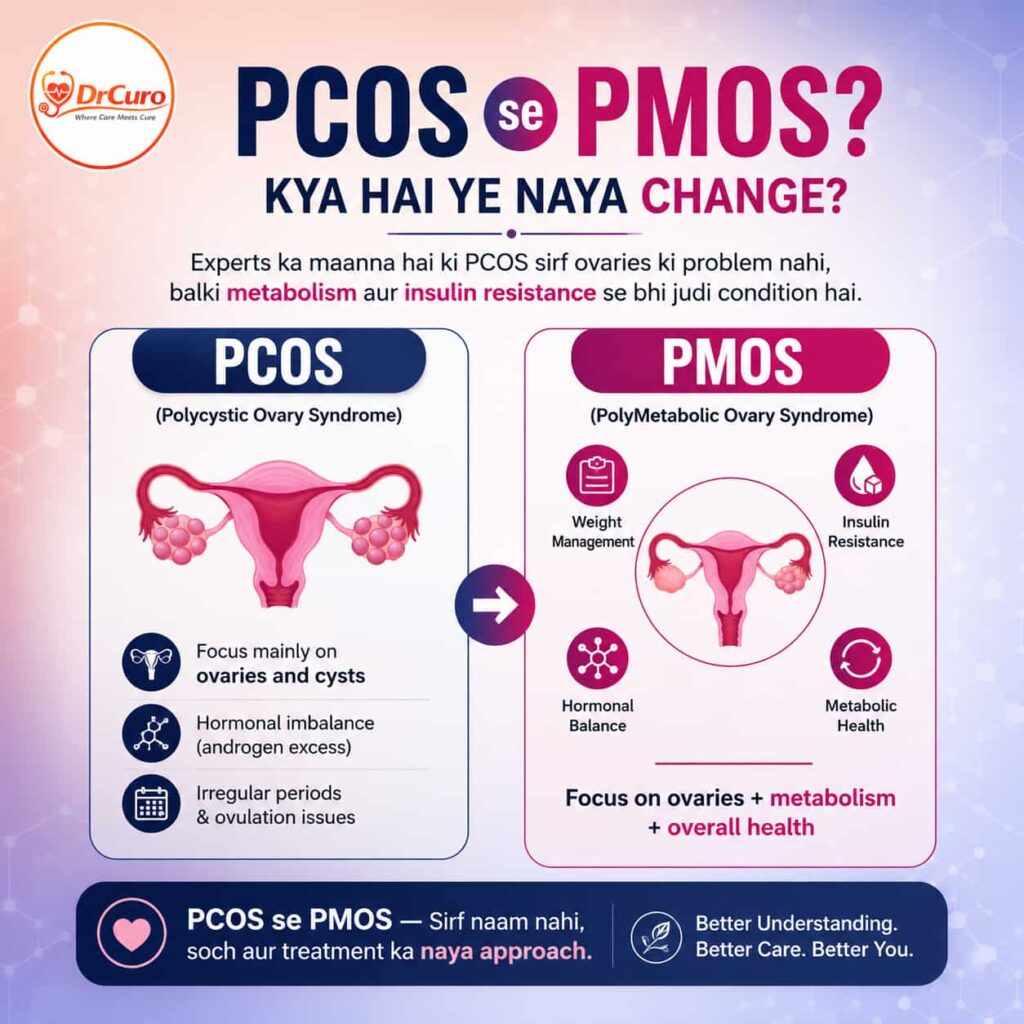
PCOS vs PMOS — A Simple Comparison
| Feature | PCOS (Old Name) | PMOS (Proposed Name) |
| Full Form | Polycystic Ovary Syndrome | PolyMetabolic Ovary Syndrome |
| Main Focus | Ovaries and cysts | Metabolism, hormones, and ovaries |
| Highlights Insulin Resistance? | Not directly | Yes — it is central |
| Addresses Whole Body? | Limited focus | Strong whole-body view |
| Links to Diabetes Risk? | Indirectly mentioned | Directly included |
| Fertility Connection | Yes | Yes |
| Weight and Metabolism | Often underestimated | Central to understanding |
| Guides Treatment Approach? | Mostly reproductive | Metabolic + reproductive |
Is PCOS Officially Renamed to PMOS? The Honest Answer
This is the question that most people want answered directly. And the honest answer is: No, PCOS has not been officially renamed to PMOS as of now. Major international medical organisations including the European Society of Human Reproduction and Embryology (ESHRE) and the American College of Obstetricians and Gynecologists (ACOG) continue to use the term PCOS in their official guidelines.
However, there is a very real and active scientific conversation happening about whether the name should be changed. Numerous researchers have published papers arguing that PCOS is a misleading and incomplete label. Some have proposed PMOS. Others have suggested names like Metabolic Reproductive Syndrome or Functional Ovarian Hyperandrogenism. No single new name has yet been universally agreed upon.
What is changing, even without an official renaming, is how doctors approach the condition. More and more medical professionals are treating PCOS as a metabolic disorder first and a reproductive disorder second. They are checking insulin levels, blood sugar, cholesterol, liver function, and inflammation markers alongside the usual hormonal tests. At drcuro, this metabolic-first approach has been at the heart of how we help women manage their condition more effectively.
The Hidden Danger — Why Metabolic Problems Are Often Missed
One of the biggest risks of the current PCOS name is that it can cause both doctors and patients to overlook serious long-term health risks. When a woman is diagnosed with PCOS, the conversation often focuses heavily on her periods and her fertility. This is understandable — these are the symptoms she is most immediately concerned about. But the metabolic problems lurking underneath can be quietly doing damage that will show up years or even decades later.
Research has shown that women with PCOS face a significantly higher risk of developing several serious long-term conditions:
- Type 2 diabetes — up to 7 times higher risk than women without PCOS
- High blood pressure, which strains the heart and blood vessels
- High cholesterol and triglycerides, increasing heart disease risk
- Non-alcoholic fatty liver disease, often with no obvious symptoms
- Sleep apnea — a condition where breathing repeatedly stops during sleep
- Higher risk of endometrial problems if periods are very infrequent
- Metabolic syndrome — a cluster of conditions that dramatically increase heart disease risk
The important thing to understand is that these are not distant, theoretical risks. They are real outcomes that affect real women and many of them can be prevented or reduced significantly with the right treatment approach. But this only happens if doctors and patients know to look for them. A name like PMOS that explicitly includes the word “metabolic” would naturally direct attention toward these risks from the very moment of diagnosis.
What Does This Mean for Fertility?
For many women, the most pressing concern when they hear a PCOS diagnosis is fertility. Irregular ovulation means that predicting the fertile window becomes very difficult. For women trying to conceive, this can be both physically and emotionally exhausting. But here is what is important to know: PCOS is one of the most treatable causes of infertility. The vast majority of women with PCOS are able to get pregnant, either naturally or with the help of treatments.
What the PMOS research has added to our understanding of fertility is that improving metabolic health often directly improves fertility outcomes. When insulin resistance is reduced through lifestyle changes, medication, or both — the hormonal chaos it creates begins to settle down. Testosterone levels may drop. Ovulation may become more regular. The body may become more receptive to fertility treatments. At drcuro, this is why we never look at fertility in isolation. We always assess the full metabolic picture, because treating the root cause gives the best chance of a healthy pregnancy.
What Can You Actually Do — Lifestyle Changes That Make a Real Difference
Whether the condition is called PCOS or PMOS, the lifestyle strategies that help women manage it remain the same. Lifestyle changes are often the single most powerful tool available more effective in the long run than many medications.
Exercise Regularly — and Vary What You Do
Exercise is one of the most powerful ways to improve insulin sensitivity. When your muscles work, they become better at absorbing glucose from the blood without needing as much insulin. Even moderate activity such as 30 minutes of brisk walking five days a week can make a measurable difference. Strength training is particularly effective because it builds muscle mass, which increases the body’s insulin sensitivity long-term. Combining cardio with strength training gives the best results.
Eat in a Way That Keeps Blood Sugar Steady
The goal with diet is not to go on an extreme eating plan, but to choose foods that release energy slowly and keep blood sugar stable. This means focusing on whole foods vegetables, legumes, eggs, fish, nuts, and whole grains and reducing highly processed foods, sugary drinks, refined flour products, and fast food. Eating protein at every meal helps with satiety and blood sugar control.
Prioritise Sleep
Poor sleep directly worsens insulin resistance and hormonal balance. Women with PCOS already have a higher risk of sleep apnea, which disrupts sleep quality even further. Aiming for 7 to 9 hours of quality sleep per night with a consistent bedtime is not a luxury, it is a health necessity.
Manage Stress Actively
Chronic stress raises cortisol levels, which in turn worsens insulin resistance and hormonal imbalance. Finding active ways to decompress whether through meditation, yoga, time in nature, creative hobbies, or therapy can have a measurable positive effect on your hormones.
Maintain a Healthy Weight — Without Obsessing Over It
For women with PCOS who are overweight, research shows that even a 5 to 10 percent reduction in body weight can significantly improve ovulation frequency, hormonal balance, and metabolic markers. However, weight loss is genuinely harder for women with PCOS due to insulin resistance so this should always be approached with kindness and medical support, not shame or extreme dieting.
Foods That Help vs Foods That May Worsen Symptoms
| Foods That May Help | Why They Help | Foods That May Worsen Symptoms | Why to Avoid |
| Eggs | Excellent protein, keeps blood sugar steady | Sugary drinks and sodas | Cause rapid insulin spikes |
| Nuts and seeds | Healthy fats that reduce inflammation | White bread and refined flour | Quickly converted to sugar |
| Green leafy vegetables | Rich in fiber and essential nutrients | Ultra-processed snack foods | Worsen inflammation |
| Lentils and legumes | Slow-release carbohydrates | Packaged cereals with added sugar | Hidden sugar, blood sugar spikes |
| Oats | Helps with steady blood sugar control | Fried and trans-fat foods | Increase cardiovascular risk |
| Fatty fish like salmon | Omega-3 reduces inflammation | Excess alcohol | Worsens hormonal imbalance |
| Berries and low-sugar fruits | Antioxidants without heavy sugar load | Excess caffeine on empty stomach | Can worsen cortisol and anxiety |

Common Myths About PCOS That Need to Be Corrected
Myth 1: Only Overweight Women Get PCOS
This is completely false. PCOS affects women of all body types and sizes. A significant percentage of women with PCOS are of normal weight or even underweight a presentation sometimes called “lean PCOS.” These women often find it harder to get diagnosed because their weight does not raise any red flags, yet their hormonal and metabolic imbalances can be just as significant.
Myth 2: If You Have PCOS, You Cannot Get Pregnant
This is one of the most harmful myths because it causes enormous unnecessary distress. The reality is that PCOS is a leading but very treatable cause of infertility. The large majority of women with PCOS are able to conceive, either naturally or with medical support. Early and correct management dramatically improves fertility outcomes.
Myth 3: PCOS Is Just About Your Periods and Ovaries
As this entire blog has explained, PCOS is a whole-body condition. It affects metabolism, cardiovascular health, liver function, mental health, skin, and hair not just the reproductive system. This myth is exactly why the proposed name change to PMOS is being taken seriously by the medical community.
Myth 4: PCOS Goes Away After Menopause
While the reproductive symptoms naturally resolve after menopause, the underlying metabolic issues — insulin resistance, increased diabetes risk, and cardiovascular risk continue. Women with PCOS need to monitor their metabolic health throughout their entire lives.
The Emotional and Mental Health Side of PCOS
At drcuro, we believe that the emotional experience of living with PCOS deserves just as much attention as the physical symptoms. PCOS can be profoundly affecting to a woman’s sense of self. Acne in adulthood, facial hair, weight gain that does not respond to diet and exercise, and the fear of infertility these experiences can lead to real and serious mental health consequences.
Research has confirmed that women with PCOS have significantly higher rates of depression, anxiety, and reduced quality of life compared to women without the condition. These mental health aspects are often dismissed or go unaddressed in medical consultations. The physical symptoms also create a cruel feedback loop stress worsens cortisol levels, cortisol worsens insulin resistance, and insulin resistance worsens the very symptoms that are causing the stress.
Recognising PCOS as a whole-body condition as the proposed PMOS name encourages also means recognising that mental and emotional health is part of the treatment conversation. Women deserve compassionate, thorough care that addresses all of these dimensions, not just the ones that show up on blood tests.
When Should You See a Doctor?
You should not wait until things feel very serious before seeking medical advice. Early evaluation can prevent long-term complications. Speak to a doctor if you are experiencing any of the following:
- Your periods are consistently irregular either very frequent or going missing for months
- You are struggling to lose weight despite eating well and exercising regularly
- You notice dark patches of skin around your neck, underarms, or other skin folds
- You have more facial or body hair than is typical for your family background
- You are experiencing significant hair thinning from your scalp
- Your acne is persistent, severe, or not responding to usual treatments
- You have been trying to conceive for 12 months without success (or 6 months if you are over 35)
- You have a family history of diabetes, heart disease, or PCOS
Frequently Asked Questions
Q1. I just got diagnosed with PCOS but I am not overweight and my periods are only slightly irregular. Do I still need treatment?
Yes. PCOS is not defined by weight or the severity of period disruption alone. Even women with mild symptoms can have significant insulin resistance, elevated testosterone, or elevated risk of long-term metabolic problems. At drcuro, we always recommend a full hormonal and metabolic evaluation regardless of how mild the symptoms appear. Early lifestyle intervention can prevent much more serious problems down the line.
Q2. I have been told I have PCOS, but my ultrasound did not show any cysts. How is that possible?
This is completely normal and a great example of why the PCOS name is so confusing. The diagnosis of PCOS is based on a combination of factors — not just the ultrasound appearance. The Rotterdam Criteria, which is the most widely used diagnostic framework, requires only two out of three features: irregular periods, elevated androgens, or polycystic-appearing ovaries. You can be diagnosed with PCOS without any visible follicles on ultrasound at all.
Q3. My doctor keeps telling me to “just lose weight” but I cannot lose weight no matter what I try. What am I doing wrong?
You are probably not doing anything wrong. Insulin resistance which is extremely common in PCOS makes weight loss genuinely harder. When insulin is chronically high, the body is in fat-storing mode rather than fat-burning mode. This is a physiological problem, not a willpower problem. At drcuro, we address insulin resistance directly through dietary adjustments, targeted physical activity, and sometimes medication like metformin rather than simply advising weight loss as though it were simple.
Q4. Can PCOS come back after pregnancy?
PCOS does not go away during pregnancy, and it does not disappear after giving birth. Pregnancy can temporarily alter some hormone levels, and some women notice certain symptoms improve after having a baby but the underlying condition remains. After pregnancy, it is important to continue monitoring metabolic health and maintaining the lifestyle habits that help manage PCOS long-term.
Q5. I am in my 40s and approaching menopause. Do I still need to worry about PCOS?
Absolutely. While the reproductive symptoms of PCOS naturally wind down around menopause, the metabolic risks do not. Women with PCOS have a higher risk of Type 2 diabetes, cardiovascular disease, and other metabolic conditions throughout their lives. At drcuro, we work with women of all ages to monitor and manage these risks, because good metabolic health in your 40s and 50s has enormous consequences for quality of life in your 60s and beyond.
Q6. Should I wait for the official name change from PCOS to PMOS before changing how I manage my condition?
Not at all. Whether your doctor uses the term PCOS or PMOS, the science behind what works is the same. The most effective management approach already incorporates the metabolic understanding that the PMOS name is trying to reflect. Focus on your insulin sensitivity, your blood sugar, your diet, your exercise, your sleep, and your mental health — and work with a doctor or clinic like drcuro that takes a whole-body view of your condition.
What Actually Matters for Your Health
The debate about whether PCOS should be renamed to PMOS is not just a medical naming exercise. It represents a fundamental shift in how the medical community understands women’s health. The old framework saw PCOS as primarily an ovarian and reproductive problem. The new framework, reflected in the proposed PMOS name, recognises it as a whole-body metabolic condition in which the ovaries are affected, but are not the whole story.
For women living with this condition, this shift in understanding is genuinely important. It means that proper management should address insulin resistance, cardiovascular risk, mental health, and long-term disease prevention not just period regularity and fertility. It means that the frustrating symptoms that women have often been dismissed about the weight gain, the fatigue, the mood changes are real physiological consequences of a real metabolic condition, not personal failures.
At drcuro, we are committed to helping women navigate their health with clear information, compassionate support, and evidence-based care. Whether the world continues to use the term PCOS or gradually adopts PMOS over the coming years, our approach remains the same: look at the whole picture, treat the root cause, and support every woman in living her healthiest possible life. You deserve a diagnosis that fully explains your experience. You deserve a treatment plan that addresses everything happening in your body. And you deserve to understand your own health in language that is clear, honest, and empowering. That is what drcuro is here for.







No Comment! Be the first one.